Meniscus tears are common in the active young adult population. Typically, the mechanism of injury involves a twisting, pivoting, or explosive maneuver followed by pain and gradual onset of swelling. Symptoms of a tear include pain, clicking or catching, and a loss of confidence in the knee. MRI is the best study to confirm a suspected meniscus tear and treatment depends on the size and location of the tear. Smaller tears in the periphery of the meniscus have a good blood supply and greater capacity to heal. These tears may be treated conservatively and/or supplemented with PRP injections. Larger tears involving the central aspect of the meniscus typically require arthroscopic surgery.
The meniscus tear can be directly visualized at the time of arthroscopy with the use of a fiberoptic camera and instruments (Figure 1). There are two ways to treat meniscus tears arthroscopically: debridement and repair. Debridement involves removing the torn portion of the meniscus and leaving behind a smooth remnant. This treatment has very little downtime with patients bearing full weight immediately following surgery and returning to sport participation in as little as 4 weeks. However, the downside is that some meniscus tissue is lost and there is a higher incidence of arthritis in the future.
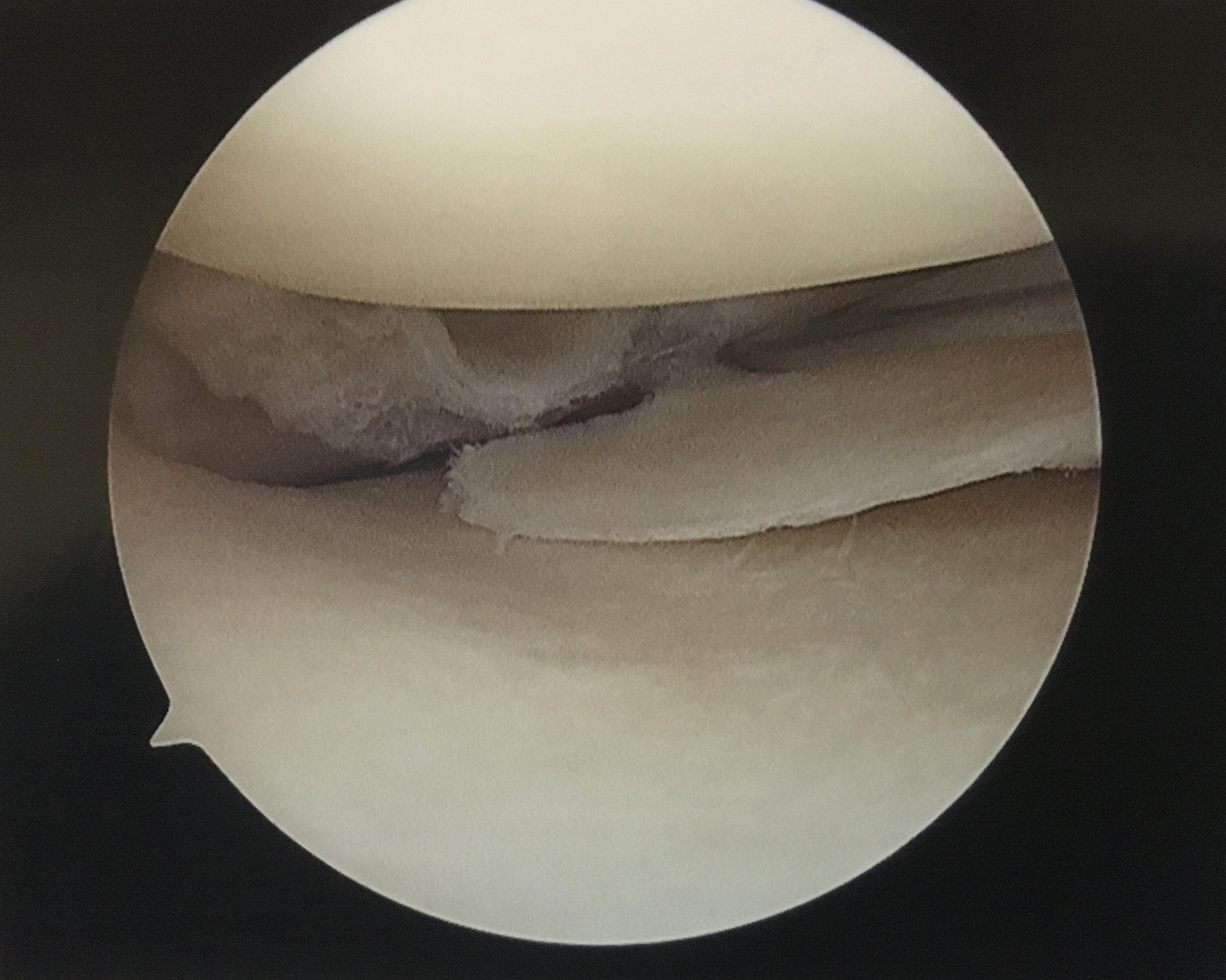
Figure 1. Arthroscopic image showing a radial tear in the posterior horn of the medial meniscus.
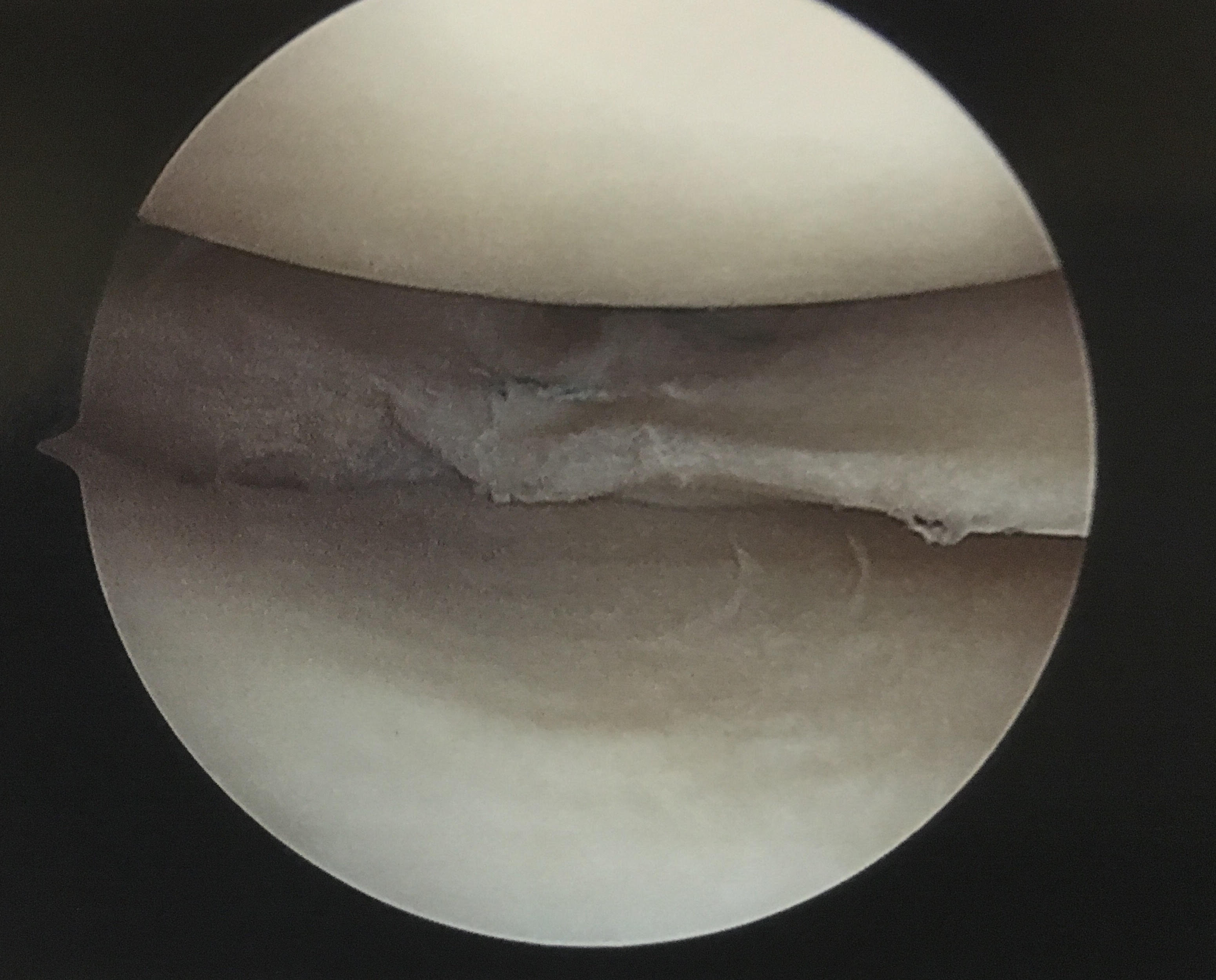
Figure 2. Arthroscopic image following repair of a meniscus tear with three anchors and side to side sutures.
Meniscus repair involves placing anchors and sutures to bridge the tear in an effort to get the body to heal the tissue (Figure 2). This treatment requires 4 weeks of crutches and an overall 2 – 3 months to return to sports participation. If the tear heals successfully, the benefits are that greater meniscal tissue will be preserved to reduce the risk of future arthritis. Not all tears are candidates for repair, however, and if the tear does not heal despite this approach then a second surgery may be necessary to debride the non-healing tissue.
Whether a meniscus tear is best treated by debridement or repair depends on a number of factors: patient age, smoker vs non-smoker, tear size/location/pattern, chronicity of injury (acute vs chronic), other concomitant injuries, quality of surface cartilage or pre-existing arthritis, and joint alignment. Often, a surgeon is prepared to perform either procedure depending on the appearance of the tissue during arthroscopic evaluation. My preference is always to preserve the meniscus with a repair, and reduce the risk of future arthritis, when the above factors collectively indicate a good chance of healing. This approach ensures that I am not just treating the current problem, but also keeping the knee healthy for years to come.
Dr. Tigran Garabekyan is a board certified orthopedic surgeon specializing in the treatment of shoulder, hip, and knee problems. To learn more about treatments provided by Dr. Garabekyan or to schedule a consultation, click here to contact us. Serving patients in Encino, Sherman Oaks, Van Nuys, North Hollywood, Burbank, Glendale, West Hollywood, Beverly Hills, Santa Monica, Los Angeles, and other neighboring cities in the greater Los Angeles area.



